

Pediatric chronic graft-versus-host disease (cGvHD) contributes to poor quality of life and increased morbidity and mortality in long term survivors of hematopoietic stem cell transplant (HSCT). Given the insidious nature of cGvHD, diagnosing cGvHD in children according to the National Institutes of Health Consensus Criteria (NIH-CC) can be challenging, particularly in the early phase of disease development. Diagnostic cGvHD biomarkers could aid in diagnosis. The Applied Biomarkers of Late Effects / Pediatric Blood and Marrow Transplant Consortium (ABLE / PBMTC 1202) study was a prospective, multi-institution study at 27 pediatric HSCT centers that evaluated biomarkers of cGvHD. Detailed clinical evaluation of cGvHD, including central adjudication when necessary, occurred as per the NIH-CC. Of the 302 enrolled children, 233 were included in this diagnostic cGvHD biomarker analysis, including 43 with cGvHD and 190 non-cGVHD controls. Peripheral blood was drawn into a STRECK tube at the onset of cGvHD and before escalation of immune suppression, sent overnight to a central laboratory, and evaluated by flow cytometry.
Five flow cytometric antibody panels consisting of 76 combinations of cell surface markers were used to delineate subpopulations of T, Regulatory T (Tregs, CD4+CD127LowCD25+), B, NK, and myeloid cells. We analyzed each marker in two ways. First, to control for normal post-HSCT immune reconstitution, we divided cGvHD subjects into early- (day 0-120), mid- (day 121-240), and late-onset (>day 240) and compared their marker values against non-cGVHD controls at day 100, 6-months, and 12-months, respectively, using fixed effect linear regression models. Second, we compared the marker values of all cGvHD subjects at diagnosis against the marker values of non-cGvHD controls at all three time points and used mixed effect linear regression models to account for within-subject correlations. A cellular subpopulation was considered a clinically relevant and potential diagnostic cGvHD biomarker if all 4 criteria were met: a) the effect ratio (mean marker value of cGvHD subjects over non-cGvHD controls) was ≥1.3 or ≤0.75, b) the p-value was ≤.05, c) the receiver-operating characteristic area under the curve was ≥0.60, and d) the marker was detected by both the mixed effect model and in the same direction across all measurement time points in the fixed effect models.
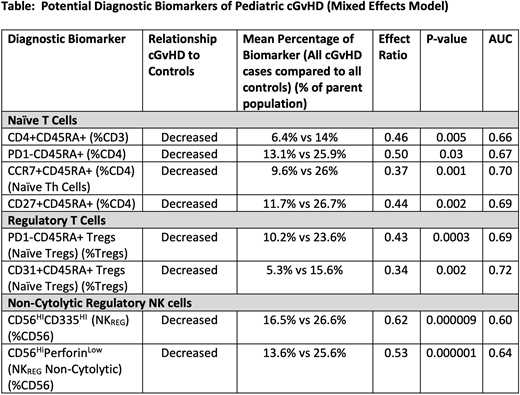
Using these criteria, 8 cellular subpopulations arose as potential diagnostic biomarkers of pediatric cGvHD (Table). Key subsets identified in cGvHD patients included decreased proportions of naïve helper T cells (CD4+CD45RA+, PD1-CD4+CD45RA+, CCR7+CD4+CD45RA+, CD27+CD4+CD45RA+), decreased naïve and recently emigrated Tregs (CD31+CD45RA+, PD1-CD45RA+), and decreased non-cytolytic regulatory NK cells (CD56BrightCD335High, CD56BrightPerforinLow). CD4+ recent thymic emigrants (CD4+CD31+CD45RA+), markers of thymopoeisis, were also significantly decreased in cGvHD (p=0.01) but did not meet all the required biomarker criteria.
Evaluation of specific subsets of pediatric cGvHD showed that CD21LowCD19+ B cells were lower in patients with pulmonary (n=12) compared to a mucocutaneous predominant phenotype (n=31) (p=0.048). Cases of progressive cGvHD (n=18), characterized by concurrent acute GvHD features (overlap syndrome), had decreased proportions of CD19 B cells, T3 transitional B cells (CD38LowCD10-) and mature naïve B cells (IgD+CD27-), decreased naïve helper T cells (CCR7+CD4+CD45RA+) and increased activated NK cells (CD56dimCD69+) (all p<0.05). No cellular subsets were associated with the number of organ systems involved with cGvHD or global cGvHD severity according to the NIH-CC.
Using a well characterized cohort of pediatric patients with cGvHD, the ABLE / PBTMC 1202 study showed that a variety of subpopulations of naïve helper T cells, Tregs, and regulatory NK cells were associated with cGvHD. Additional B-cell markers were associated with progressive cGvHD in children. These data support alterations in thymopoeisis and decreases in regulatory T- and NK-cell populations underlying pediatric cGvHD. Future work includes the addition of non-cellular plasma markers into a clinically applicable diagnostic biomarker algorithm to aid clinicians in the accurate diagnosis of pediatric cGvHD, as well as further validation in the ABLE 2.0 / Pediatric Transplant Cellular Therapy Consortium 1901 study.
Wahlstrom:Pharmacyclics: Current Employment. Pulsipher:Mesoblast: Honoraria; Adaptive: Research Funding; Miltenyi: Honoraria, Research Funding; Bellicum: Honoraria; Jasper: Honoraria; Novartis: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal